Without figures for Newfoundland ... from a Canadian Government post-war publication ...
about 2400 Canadian nurses went overseas with the Canadian Expeditionary Force and served in
England, France, Belgium, Egypt, Greece and Russia.
Of these, 37 died : at sea (a Canadian hospital ship was sunk), or overseas of wounds or disease.
Battlefield survivors with limb amputations
To try to understand physical war wounds,
using an example which is at least easy to picture,
one could consider the 'limb amputations' as a group.
Canadian documents provide some idea of what might have been happening in
the health care system
of Newfoundland and in the systems of 'the other cats' to meet the health care needs of war survivors.
Initially, there was no domestic manufacturer of artificial limbs in Canada.
In the April 1916 'Special Bulletin of the Military Hospitals Commission of Canada',
it was stated by the investigator looking at artificial limbs (limb prostheses):
"It must not be forgotten that the loss
of a limb not only maims a man but, in most cases, reduces his total
physical ability. The first step in this connection would be the
transfer of the supply of the artificial limbs from the Militia
Department to this Commission and the establishment of a central depot,
either in Montreal or Toronto, where the best orthopedic advice is
available and where vocational training could be given to the men while
waiting for their limbs.
"In many workshops that I have visited, men only wore their limbs when
going to and from the workshops. Many cases can be materially assisted
by artificial appliances, but it is not advisable to make the men
dependent upon these any more than is absolutely necessary. The
supplying of complicated artificial limbs is not desirable."
Thousands of Newfoundlanders joined the Newfoundland Regiment
to 'take a crack at the Hun' and support the Empire.
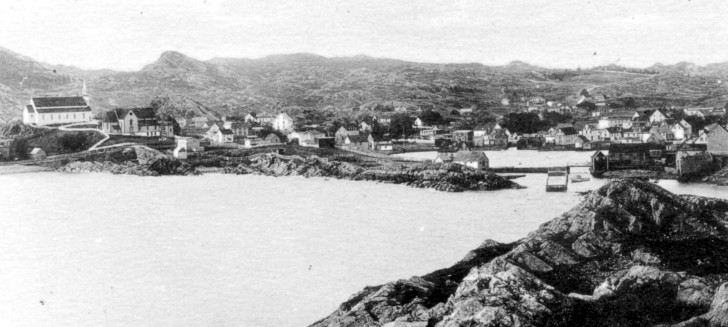
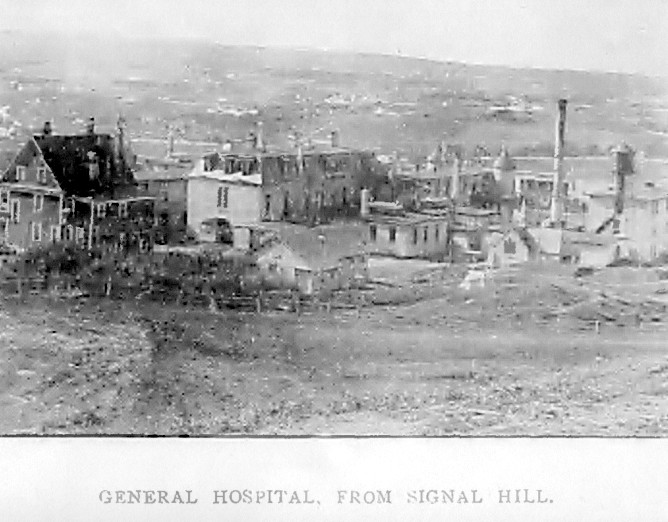
As this contemporary view of a major St. John's hospital shows ...
there will probably be a shortage of health care capacity when Great War survivors return.
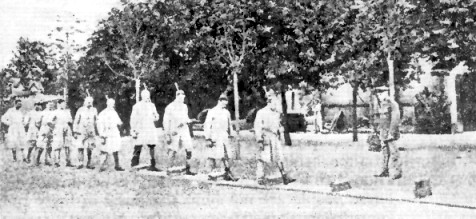
In an American textbook 'How Germany Cares for War Disabled - Lessons from the Enemy' (1918)
a photograph shows a systematic military approach to restoring the fitness of amputee soldiers.
Amputees with prostheses practice walking over obstructions while 'shouldering arms' under the supervision of an officer.
Another photo shows some soldiers hurdling with prostheses.
It is not clear how universal these efforts were.
Perhaps in Germany where major wars seemed rather ... frequent ...
it made sense for the state to have a more 'hands on' approach
in managing the rehabilitation and productive occupation of war amputees.
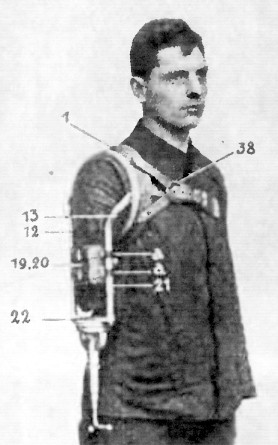
Complicated, compared to Canadian prosthetic recommendations above,
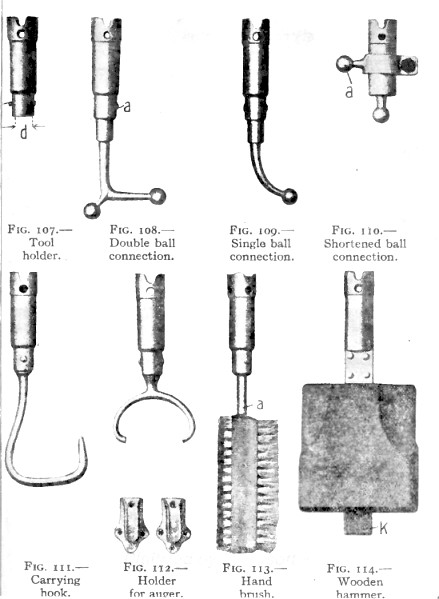
the various adjustments for a German 'work arm' are shown.
Germany had previous experience in caring for war amputees, with its population generally close to large urban centres.
Because of war losses, Germany had a relative shortage of male labour,
so there was a strategic advantage in maintaining the industrial productivity of its war amputees.
Canada did not have these characteristics.
 Filing metal parts
Photos of the German workers show them ...
Filing metal parts
Photos of the German workers show them ...
planing, scraping, working at drafting plans, hammering,
nailing, and washing the other hand with a brush attachment ...
To repeat the Canadian recommendation of 1916 ...
"In many workshops that I have visited, men only wore their limbs when
going to and from the workshops. Many cases can be materially assisted
by artificial appliances, but it is not advisable to make the men
dependent upon these any more than is absolutely necessary. The
supplying of complicated artificial limbs is not desirable."
Phantom Limb Pain
In 1915, Wilfred Harris, physician
to St. Mary's Hospital, London, and to The Hospital for Epilepsy and
Paralysis ... was working as a captain in the Royal Army Medical Corps
at the 3rd London General Hospital, which is mentioned later on this
page in connection with Newfoundland and Canadian patients.
He put together a booklet entitled "Nerve Injuries and Shock" in the "Oxford War Primers" series.
"The hysterical cases are usually
to be distinguished from true painful neuroma by the exaggerated
condition of hyperaesthesia present, affecting large areas of skin,
which should not be tender in neuroma. Any movement, moreover, is
likely to cause apparent pain in the hysterical painful stump.
Inconsistence of the patient with regard to his pain will usually give
away his case. Thus I have seen a man, who had amputation performed
through the middle of his forearm on account of an injury, develop
intense pain in the stump a week afterwards, the flap being opened and
explored by the surgeon after a fortnight. Nothing was found to account
for this pain, and he was sent out of hospital, being told to wear his
arm in a sling and protect it carefully. A fortnight later this man
walked up from Maidenhead twenty-six miles to St. Mary's Hospital, with
his arm swathed in cotton wool at least two inches thick, and carrying
his arm in a sling on account of the intense tenderness any touch or
movement provoked, as he said. Yet the very fact of his being able to
walk with his arm in that condition proved beyond a possibility of a
doubt that the tenderness was psychical and not physical. After
unwrapping his limb nothing abnormal was found, though the man
complained of intense hyperaesthesia for any touch or movement.
However, firm treatment with faradism and the wire brush, combined with
suggestive encouragement, dissipated the hyperaesthesia entirely and
cured him of his trouble in less than five minutes."
The patient must have been well-motivated by something to walk 26 miles to a doctor's appointment.
I can't tell you if this is a case of phantom limb pain or not.
Certainly this story suggests the difficulties which 'working class' British
patients - educated 100 years ago without today's knowledge of the
nervous system - would have if their symptoms were different from those
anticipated by an 'expert' medical officer.
If an arm or leg was amputated in 1915 ... but the patient sometimes
still felt the limb there - as if whole again ... and often felt great
pain within the absent limb ... the patient might
decide their sanity was being lost. In addition, chronic pain can often
cause depression ... which, in turn, can make the pain worse. This
would have been a treatment
nightmare in 1915 for even an open-minded doctor with an abiding
'interest' in the patient's progress.
To be fair, in his book Captain Harris has only about 125 pages to cover the wide
range of physical nerve injuries which can occur during war, so the
fact that 'phantom limb pain' is not addressed at all in his book
should not be too disappointing ... I guess.
The human nervous system is complex and wonderful and
evolved over millions of years. It still has many secrets from medical
science.
Young American military patients on TV documentaries of the 21st
Century have stated that it feels as if their amputated arm is still present and burning
in a fire, or is being actively crushed in a vice. No one knows
precisely what
explains phantom limb pain ... or how to treat it with complete
success.
Intuitively, one would assume it must be triggered by the damaged
nerves at the stump as Dr. Harris confidently states for the
'non-hysterical' cases of stump pain.
However, it seems more likely with today's knowledge ... that 'garbled
signals' from the stump may interact somehow with the many nerve
junctions at the spine, sending out an amplified cascade of 'bad pain
signals' ... or maybe the secret of chronic phantom pain is
somewhere in the 'mapping' of the whole body and its peripheral nerves
inside the brain.
You can also imagine there are stress hormone
'signals' floating around in the body's chemical soup to make the
symptoms worse.
Whatever causes intense phantom limb pain ... perhaps Dr. Harris
overwhelmed the 'garbled signals' for a while with his electrical
stimulation and the wire brush.
So to imagine a really depressing case ...
a soldier volunteered to do his part,
had a limb destroyed in battle,
then he got a poor-quality government issue prosthetic,
and he seems to be crazy, because he is 'imagining' phantom limb pain,
... and, in addition, the experience of chronic pain is making him depressed.
In lieu of adequate attentive medical care back in 1915,
he can always drink alcohol, which will dull the pain for a while ...
whether the phantom pain originates at the stump, the spine, the brain - or all three for that matter!
But ... he'll need more and more alcohol to have the same effect ...
... and the alcohol itself will make the veteran's depression even worse over time ...
Youth of the Empire ! ...
My simplistic 'cartoon' ...
a 'patriotic message' for battlefield survivors ...
The innocence of youth is first exposed to the horror of the battlefield,
then to the horror of cost containment through bureaucracy.
Thank you so much for your recent idealistic and patriotic enlistment into
the armed services of His Majesty.
First the good news : We shall be victorious ! ... someday ... when we beat the Wiley Hun.
Awfully sorry about your friends and sibling(s) getting killed in
the shellings and attacks ... bad show, that ... nonetheless, we Celebrate our Glorious War Dead!
Their problems are over and yours have just begun ... um, rather ... very sorry to hear about your life-changing injuries.
As you know, the War is full of surprises
for all of us ... and we Leaders of The War haven't escaped scot-free either, you know :
... We must now struggle to cope with the problems You Wounded are
creating for Our War Effort. What a bloody inconvenience 'wastage' is!
Let us consider your Canadian House of Commons Special
Committee on the Care and Treatment of Returned Soldiers, from July 1917 ...
"Your Committee has very thoroughly investigated the matter of the care
and treatment at present being given to wounded soldiers, but has not,
as yet, given an exhaustive study to the problem attendant upon
demobilization and 'liquidation' of the war."
So 'cheer up', 'chin-chin', 'pack up your troubles' and all that ... after
you are discharged and financially 'fixed' with a pension ... the war
will soon be liquidated and we can all get back to normal life. Won't that
be grand? ...
Returned to Canada by April 1917.
Disability as fixed by Medical Board at disembarkation port.
|
Number of
Soldiers
|
Up to 25 % disability
|
7,418
|
26 to 50 % disability
|
2,923
|
51 to 75 % disability
|
927
|
76 to 100% disability
|
1,975
|
583 cases - 'no record'
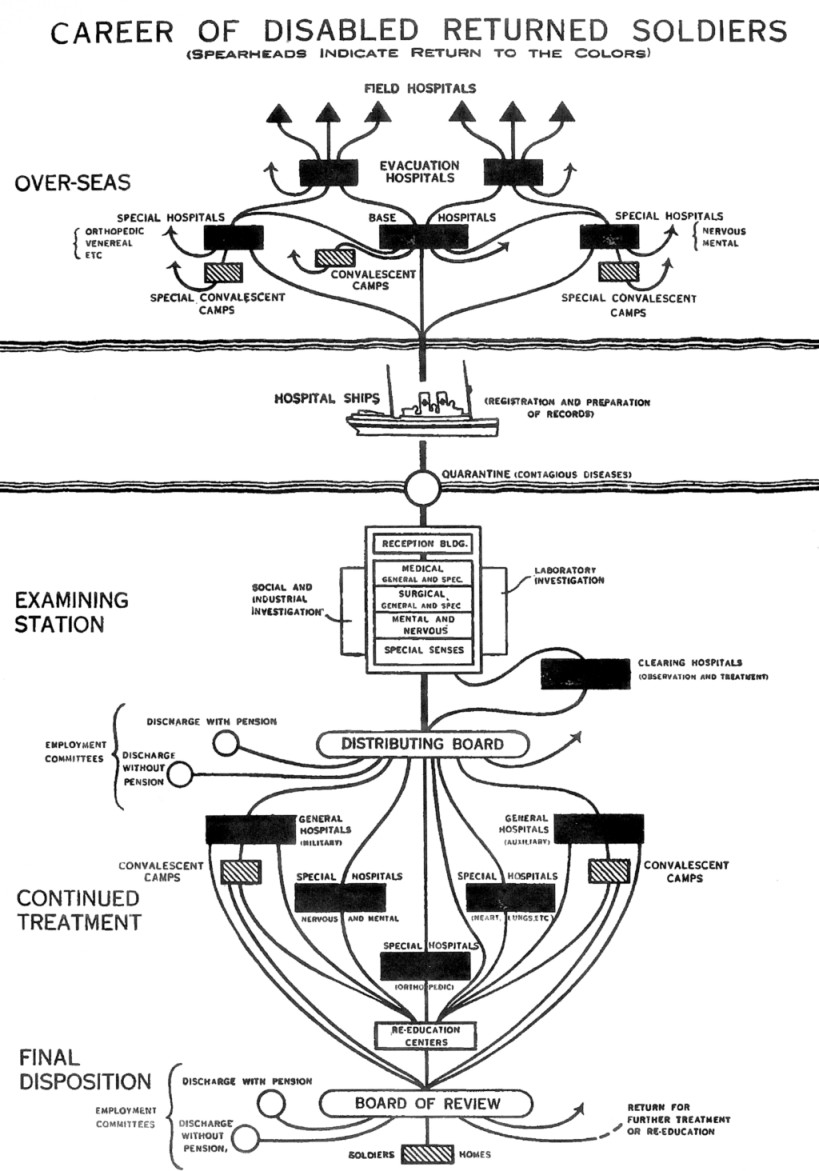
... and you will no doubt be proud to learn that the Americans have been studying and learning from our developing British
system. Below is a flow chart they made of our processes in 1917 for
their own military administration and politicians (we requested a copy because it looks so good on paper)
...
... sorry again about your life-changing
injuries, the U-boat terror you may feel on the way back across the
'Pond', the military
discipline and commotion of your 'rest' period, and all the medical
officers, and 'boards', and bureaucracy, you are enduring in your state
... and the additional anxiety all this may cause you ...
Godspeed to your happy 'Final Disposition' in Canada at the bottom of the chart.
We know you have a choice of empires to fight, die, and devastate your future plans for
...
thank you for choosing The British Empire and we hope to see you
again*.
* Once per annum maximum ... on Remembrance Day ...
You see ... if voters (and women) understand that war maims and cripples people ...
it will be hard to promote the important idea that EVERY future war is a 'necessary' war for 'freedom'.
Remember: Don't complain and make nuisance of yourself ... there's a good soldier ...
God Save the King !
Here is an American administrative textbook's flow chart of British processes, 1917 ...
there was no 'handout' for Empire (e.g. Canadian, Newfoundland) wounded to explain the process they were going through.
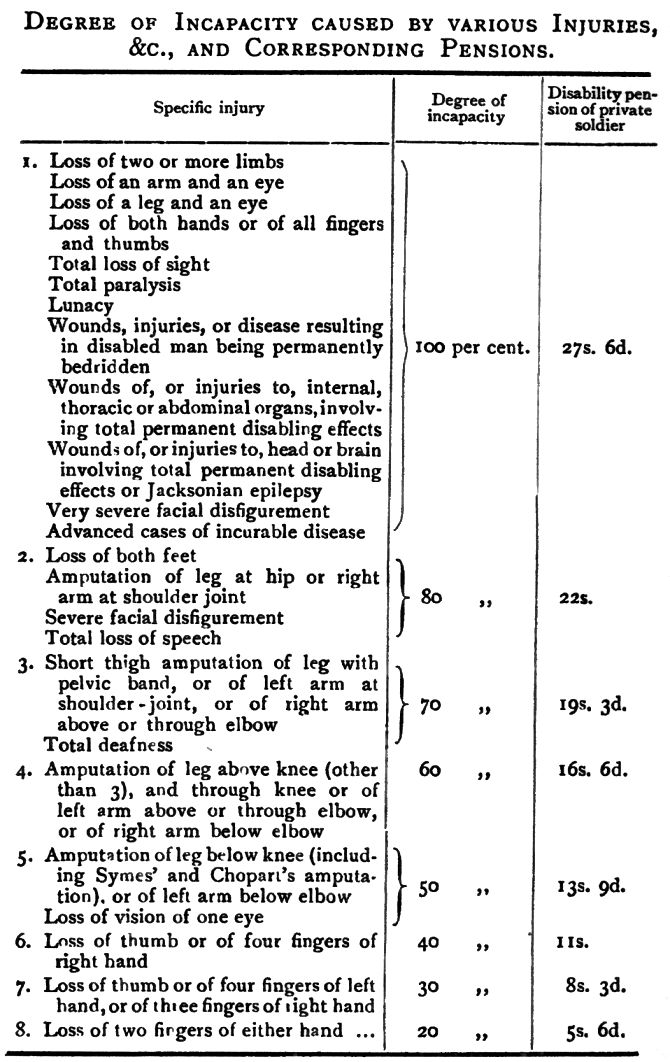
 Below is the Britsh schedule for calculating ' % disability ' for disability pensions.
Below is the Britsh schedule for calculating ' % disability ' for disability pensions.
No similar document for Canadian Great War pensions has turned up.
Keep in mind regular 'service pensions' would also be paid.
Treatment of wounded 'Dominion' troops in general ...
'Politics and the CAMC'
CAMC
was the Canadian Army Medical Corps, including people such as physician
and field surgeon John McCrae, the author of 'In Flanders Fields'.
RAMC was the Royal Army Medical Corps - the senior medical
service (British) for the Empire troops fighting in Europe and in the
other theatres such as Greece, Turkey, Italy, Palestine, Mesopotamia, etc.
 Postcard of the port of Corfu - part of the Salonikan Theatre of war.
Postcard of the port of Corfu - part of the Salonikan Theatre of war.
About 500,000 Allied troops fought in the area, including British and French units.
Our Serbian allies (... yes!) fled to this island after the Austro-Hungarian/German invasion of Serbia
and the overland death march of its population to escape.
(94,000 Serb soldiers killed; 174,000 captured or missing; civilian death toll unknown)
After the battle known as Second Ypres in April 1915, the Canadian
government found it politically necessary to send a Colonel Bruce of
Toronto to investigate the CAMC and formulate recommendations. In the time-honoured Canadian tradition of 'critics be quiet ... we are studying the issue' the Government bought itself some time.
Whether Colonel Bruce was right ... with his report which made many powerful people look as if they were building their careers and supporting the war - but not the troops...
or whether he was a prima donna surgeon ... might be open to
debate by some. He presented his confidential report on September 20,
1916. Bruce and his fellow investigators believed that their
observations should have been used to improve
care ... but they also must have known that their report could be used as a political football if
the confidential recommendations were made public ... and of course
they were ...
In fact, his
criticisms were framed by some as disparaging the sincere and
sacrificing John McCraes of the war ... largely this was probably done to draw
attention away from the
failures of those in power. The politicians
punished him and his supporters ... then quietly cherry-picked most of his
recommendations. As his 1919 career summary below indicates, he didn't
need the headache of Canadian 'government work' to earn a living or get
recognition for his abilities ...
Colonel Herbert A. Bruce, MD, FRCS, was Associate Professor Clinical
Surgery, University of Toronto; and Surgeon at the Toronto General
Hospital. He was also Past President of the Toronto Academy of
Medicine; Regent of the American College of Surgeons, Washington;
Fellow of the American Surgical Association, Vice-President of the
Congress of Clinical Surgeons of North America, and former President of
the Ontario Medical Association.

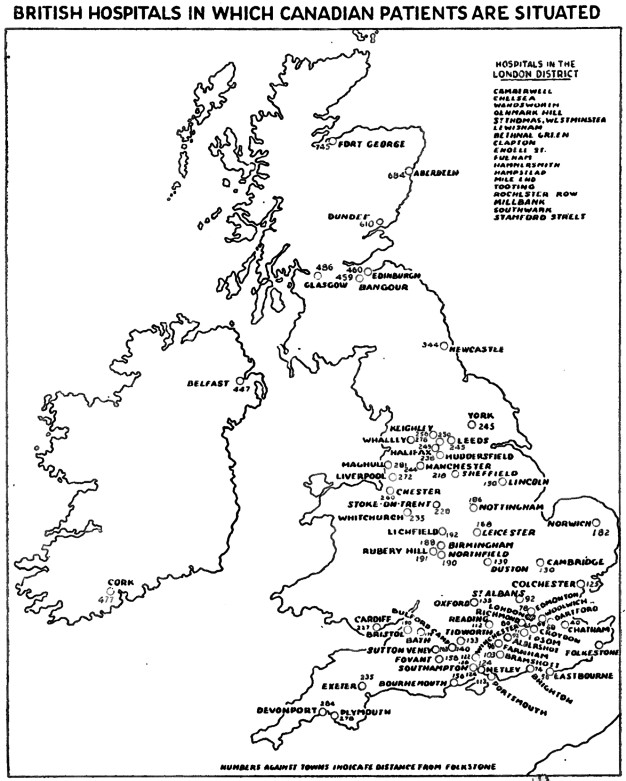
If you are going to review the care of a patient population - i.e.
wounded Canadian soldiers - first you must have a look at them.
This is where Dr. Bruce had found them ...
Numbers represent miles from Folkestone - the closest point to France.
Some details from the Bruce Report ...
Canadians were discovered to be in 800
different British hospitals!
- Who knew? Well ... no one ... as
there was no central registry of Canadian patients.
- Repeatedly, the Canadian authorities were making offers of
medical/surgical help to the Imperial and French governments. Hector
Charlesworth (a Toronto newspaper editor) suggested "It is not an unfair inference that an appetite
for titular honors and other distinctions lay back of this policy."
That is, the possibility of getting knighthoods from the British, and
state medals from the French, influenced the decisions of those who made these offers and assigned
CAMC medical professionals.
- Charlesworth also wrote that the report ... "Had its reflex in
Great Britain, where it was made to appear that the 'Bruce Report' was
a deliberate assault on the sacred cause of Imperialism and an affront
to the unselfish young women who constituted the Voluntary Aid
Detachment." In many cases VAD hospitals were poorly-equipped, large private
dwellings staffed primarily by volunteers without medical training who 'learned
on the job'. Canadians and Newfoundlanders in VAD facilities were often
attended by local civilian doctors without surgical experience.
- Keep in mind that in 'The Great War' soldiers were needed to get better and fight again ...
or should have been returned home to Canada when they were stable enough to travel.
- The Canadian government paid 90% of the cost of many designated VAD hospital beds whether they were occupied or not.
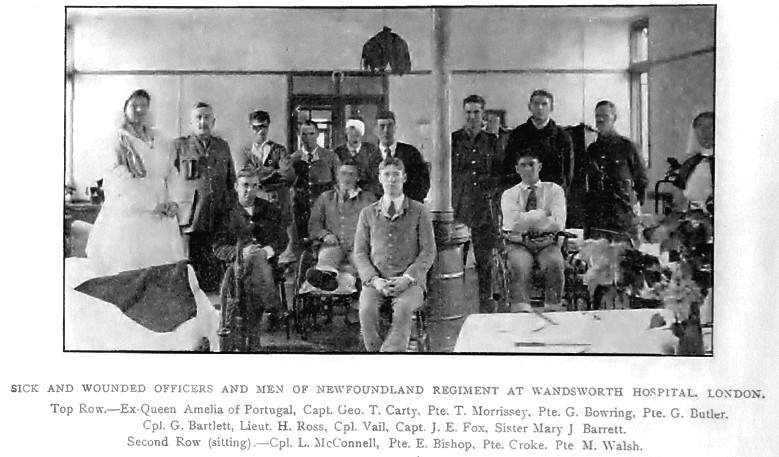 According to the map above, Canadians were also patients at Wandsworth (not a VAD facility).
According to the map above, Canadians were also patients at Wandsworth (not a VAD facility).
Originally a Victorian school for orphan daughters of British military personnel,
Wandsworth was quickly converted to the '3rd London General Hospital' to handle Great War wounded.
Selected Bruce Report findings continue ...
- The first responsibility of the CAMC - in Bruce's opinion - was to
provide care for sick and wounded Canadian soldiers. When his report
was published, 3 complete Canadian hospital units with a bed capacity
of 2800 were in Salonika (postcard above) where no Canadians were serving.
- Because of poor military medical screening in Canada, soldiers who
should never have been sent to war, including many with active tuberculosis,
were in Europe.
- There had been no Canadian inspection of Canadian patients
... some were in hospital one year after they should have been
discharged ... while others were shifted from hospital to hospital (there
were plenty to chose from) without satisfactory medical records. Of
course, for efficacious treatment for the patient's sake, one should
keep accurate medical records. If disabled soldiers were to be pensioned
by the Canadian government for the rest of their lives, records of
treatment would have been nice to have. "The records of the sick were found to be
hopelessly bad, patients were rarely bringing with them any written
information from France, and very insufficient and unsatisfactory
records were being kept in England. The entry on the medical history sheet
(the only record in most cases) was made, as a rule, by the registrar
of the hospital, who knew nothing whatever about the patient, saw him
only on admission and discharge, and blindly copied the diagnosis
already entered on the medical history sheet at the previous hospital,
or jotted down whatever the patient stated to be his disability."
- Medical review boards were often hastily assembled, with new
physicians who had no experience treating battlefield injuries assessing
the cases.
- Canadians were being held in British hospitals for limb
prostheses which were being ordered, manufactured and shipped from the
U.S.
- Dr. Bruce uncovered one case where a Canadian amputee was shipped back to Britain, from Canada, to receive his American-made artificial limb.
End of details from the Bruce Report.
To summarize some of Dr. Bruce's points :
- Canada had sent soldiers and medical professionals to The
War, with the latter group generally believing they would be taking care of 'our troops'.
- Wounded Canadians should have been streamed from France, to
southern England, and the disabled sent home to Canada as soon as the trip would not harm
their health.
- For reasons of accurate record-keeping, and the morale and mental health of
patients surviving the battlefield and traumatic injury, and to support later care and to
document pension claims in Canada ... Canadians should have been
treated by Canadians in Canadian-run military hospitals ... according to Dr.
Bruce.
- Food, fuel, and human resources were in short supply and
expensive for Canada to purchase in Britain. Food and fuel often had to run a
gauntlet of German U-boats. It was very inefficient and expensive to
treat badly wounded Canadians by shipping them around aimlessly ...
rather than 'voting them off the island' as soon as possible!
There are at least two possible reasons to explain the conditions to which Dr. Bruce took exception ...
- Very little about the Great War was foreseen and planned for.
The need for health care, and particularly psychological care,
initially were war
fighting 'frills' ... unlike the priorities for 'victory' and/or
protecting
the stability of ante bellum power structures [wow, I wrote that!] So the Big Priorities which received the most
leadership attention and resources were ... maintaining the Empire's
status, and colonial possessions, and international alliances ; war
'strategy' and weapon production, and paying companies for producing
the weapons; raising and training massive
volunteer armies and supplying them with food clothing shelter
transportation weapons and officer leadership. It
is no wonder that health care of the soldiers was a mess ... it was
just too low on the long list.
- The Empire's Leaders ran things and set the expectations for the Dominions.
For example, considering the Newfoundlanders and
particularly the Canadians ... Field Marshal Sir Douglas Haig's 500 page diary
yields the following
typical Imperial perspective. After the Commander-in-Chief of the
British forces (Haig) was formally asked that Canadian units be
allowed to fight together as a 'Canadian army' ... Douglas Haig wrote: "I
could not help feeling that some people in Canada regard themselves
rather as 'allies' than fellow citizens of the Empire!" ...
Realistically then, what were the chances that Empire leaders would let
Canadian medical personnel focus on treating the Canadian soldiers?
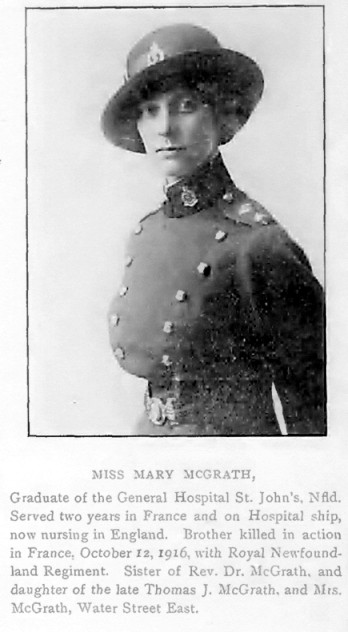
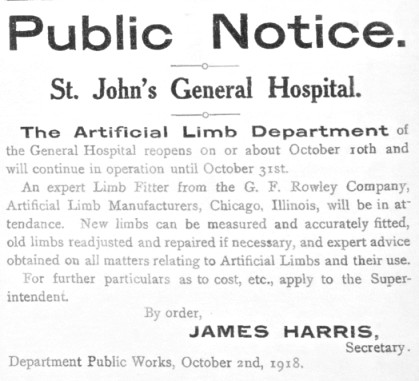
This notice in The Newfoundland Quarterly - at the end of the war -
first got me interested in reading about some of the experiences and 'health outcomes' for battlefield survivors.
The View of a Subaltern at the Front

I don't have a picture of the soldier who wrote the following poem,
so here is Lieutenant Reid again to represent 'middle management'.
If you were a military mail censor,
(usually an administrative officer or a chaplain)
with the responsibility of:
1. protecting military information
2. monitoring the general morale of the troops through their mail
How might you assess Lieutenant Murphy's health?